


- Abuse & The Abuser
- Achievement
- Activity, Fitness & Sport
- Aging & Maturity
- Altruism & Kindness
- Atrocities, Racism & Inequality
- Challenges & Pitfalls
- Choices & Decisions
- Communication Skills
- Crime & Punishment
- Dangerous Situations
- Dealing with Addictions
- Debatable Issues & Moral Questions
- Determination & Achievement
- Diet & Nutrition
- Employment & Career
- Ethical dilemmas
- Experience & Adventure
- Faith, Something to Believe in
- Fears & Phobias
- Friends & Acquaintances
- Habits. Good & Bad
- Honour & Respect
- Human Nature
- Image & Uniqueness
- Immediate Family Relations
- Influence & Negotiation
- Interdependence & Independence
- Life's Big Questions
- Love, Dating & Marriage
- Manners & Etiquette
- Money & Finances
- Moods & Emotions
- Other Beneficial Approaches
- Other Relationships
- Overall health
- Passions & Strengths
- Peace & Forgiveness
- Personal Change
- Personal Development
- Politics & Governance
- Positive & Negative Attitudes
- Rights & Freedom
- Self Harm & Self Sabotage
- Sexual Preferences
- Sexual Relations
- Sins
- Thanks & Gratitude
- The Legacy We Leave
- The Search for Happiness
- Time. Past, present & Future
- Today's World, Projecting Tomorrow
- Truth & Character
- Unattractive Qualities
- Wisdom & Knowledge




FOLLOWERS
0
Users
Outlooks & Setbacks Saturdays
Scars From Self-Harm
One of the babysitters that I use fairly frequently has quite a few scars from self-harm. They are mostly on her arms and thighs.
I really admire that she doesn’t let these scars stop her from wearing shorts or short sleeved shirts. The scars are very obviously scars from self-harm and I know that a lot of people would be embarrassed for others to see these and recognize where they came from. She just owns it and carries on.
The thing about self-harm is that certain types of self-harm cause scars - like cutting. Other types of self-harm like alcohol abuse do not. So when people have scars from self-harm, it is a constant visual representation of what they are struggling with.
I have never engaged in self-harming behaviors - but I know that many people in the world today are struggling with this.
I want you to know that if you are struggling with any form of self-harm - whether it causes scars or not - that it is ok to seek help. In fact, it is necessary that you seek help because you can learn skills and access resources that will help you with your mental health. Seeking help might seem scary, and you might have to search for the right therapist, but it will be worth it in the long run.
If you have scars from self-harming behaviors, please do not feel ashamed. We all struggle with different things in our lives, and it’s about learning how to be resilient in the face of stress.
Interesting Fact #1
Dialectical behavior therapy (DBT): In this kind of therapy a psychologist works with your child to help her learn how to tolerate uncomfortable feelings like anger, anxiety and rejection without resorting to cutting.
Interesting Fact #2
Cognitive behavioral therapy (CBT): In CBT, a psychologist teaches your child to recognize and challenge negative, distressing thoughts, and train herself to think outside of them.
Interesting Fact #3
It is not done to get attention or be dramatic Individuals that hurt themselves often try to hide their behaviors, because they are ashamed. These behaviors are most often used as a method to handle stress, and not because these individuals want more attention.

Quote of the day
“The most fundamental aggression to ourselves, the most fundamental harm we can do to ourselves, is to remain ignorant by not having the courage and the respect to look at ourselves honestly and gently.” ― Pema Chödrön
Article of the day - Self-Harm Statistics
Though self-harm is not a mental health disorder, it is often a symptom of other conditions, which makes understanding self-harm facts and statistics essential.
Self-harm involves a person damaging their body by cutting, burning, scratching or practicing any other behavior that results in pain or injury. Different motivators can encourage people toward self-harm, such as feeling overwhelmed or numb. Thoughself-harmis not a mental health disorder, it is a common symptom of many psychological conditions. Self-harm statistics and facts show the widespread trend of self-harm throughout the United States.
Article at a Glance:
- Self-harming behaviors include cutting, burning,andscratching oneself.
- The rates of self-harming behaviors are likely much higher than the statistics actually reported.
- Teens have the highest rates of self-harming behaviors.
- Self-harming behaviors are often co-occurring with eating disorders and substance abuse.
- Self-harm is not a mental health condition in itself, but treatment is available if self-harm is connected to drug and alcohol abuse.

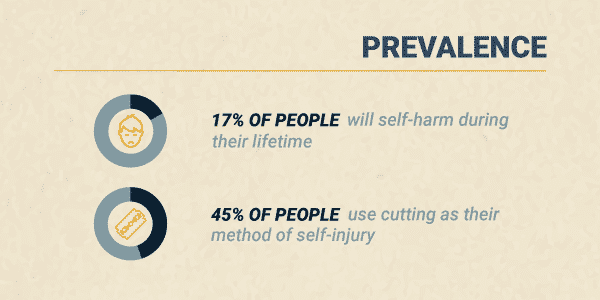
Self-Injury Prevalence
Even though self-harm has been studied extensively for over a decade, findings are never entirely accurate because of the stigma and shame that still surrounds self-injury. The actual rates are likely quite higher than those currently reported.
One analysis of self-injuryacross more than 40 countries found that:
- About 17% of all people will self-harm during their lifetime
- The average age of the first incident of self-harm is 13
- 45% of people use cutting as their method of self-injury
- About 50% of people seek help for their self-harm but only from friends instead of professionals
Not only is self-harm prevalent, but rates are increasing. According toemergency room trends, there’s been a 50% increase in reported self-injury among young females since 2009.
Who Self-Harms?
While anyone can practice self-harm, rates tend to differ among certain populations:
- Adults. Aside from very young children, adults are the least likely group of people to follow through with self-injury. Only about5% of adultshave self-injured in their lifetime.
- Teens. Adolescents have the highest rate of self-injurious behaviors, with about17%admitting to self-injury at least once in their life.
- College Students. Studies find that about15%of college students report engaging in self-harm.
- Women vs. Men. While women are more likely to self-harm, males may represent at least35%of total self-injury cases. Men are more likely to underreport self-injury and have other people hurt them than women.
- Sexual Minorities.Gay and bisexual peopleare at a high risk of self-injury.Nearly halfof all bisexual females engage in self-injury.
Age of Onset
As mentioned, the average age of onset forself-injuryis 13. This age seems to align with new stressors and expectations at school and home as the child enters their teenage years. Age 13 represents a time of great physical, social and mental change and development. This time is also linked to the emergence ofmental health conditionslike anxiety and depression, which may further trigger a desire to self-harm.
Related Topic:How long does depression last?
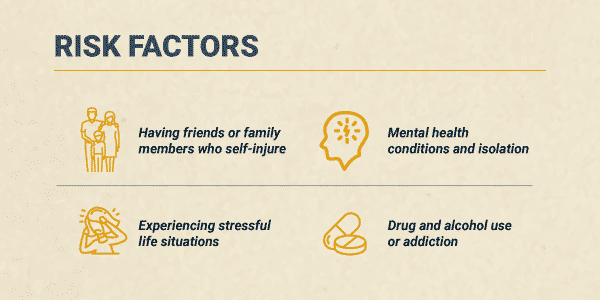
Self-Harm Risk Factors
There is not just one factor that contributes to self-harm. Instead, there are a variety of biological and environmentalissues known to cause self-harm, including:
- Having friends or family members who self-injure
- Experiencing stressful life situations like traumatic events, family instability and sexual identity uncertainty
- Living in social isolation
- Mental health conditions, likedepression,anxietyandpersonality disorders
- Drug and alcohol use oraddiction
The more of these factors a person has, the higher their risk of self-harm.
Diagnosing Nonsuicidal Self-Injury Disorder (NSSID)
Nonsuicidal self-injury is not a diagnosable mental health condition: yet. Currently, the American Psychiatric Association (APA) lists nonsuicidal self-injury as one of the “Conditions for Further Study” in the most recent Diagnostic and Statistical Manual of Mental Disorders (DSM-5). This designation implies the group may include the condition in future versions of the text.
Nonsuicidal self-injury involves symptoms like:
- Engaging in self-harm on five or more days over the last year
- Self-injuring to find relief from an unwanted feeling, solve a relationship conflict or create a desired feeling
- Self-harm involves unwanted feeling like depression, anxiety or anger, an intense focus on completing the behavior and frequent thoughts of self-injury
Since self-injury is not currently an official mental health diagnosis, a medical or mental health professional will ask the person questions about the behavior and the purpose of the behavior to assess the situation.
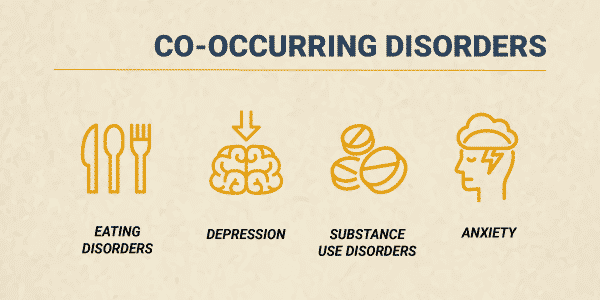
Rates of Self-Harm and Co-Occurring Conditions
Self-harm often co-occurs with mental health disorders. Historically, self-harm was thought to be directly connected toborderline personality disorder. Now, it’s understood that the behavior can be associated with many conditions, like:
Onestudy foundthat of people who self-injure:
- 20% have personality disorders
- 13.5% have adjustment disorders
- 11% have mood disorders, like depression or bipolar disorder
Addition research shows that about55%of people who self-harm have eating disorders.
Although the conditions may overlap, nonsuicidal self-injury is often not linked to:
- Obsessive-compulsive disorder(OCD)
- Excoriation(skin-picking) disorder
- Trichotillomania(hair-pulling disorder)
Self-Harm and Suicide
Although an act of self-harm is different from a suicide attempt, there is a strong association between self-injury and suicide attempts. It seems that as incidents of self-harm increase, the likelihood of suicide attempts also increase.
People who engaged in 20 or more self-harm behaviors are about3.5 times more likely to attempt suicidecompared to those who have fewer self-injury actions.
Self-Harm Prognosis
Establishing a self-harm prognosis is based on:
- Frequency of self-harm
- Intensity of self-harm
- Duration of self-harm
- Presence of other mental health symptoms or conditions
- Available professional or social support
The APA reports in the DSM-5 that self-injury tends to peak by the time a person is 29, so the prognosis improves as age increases.
Statistics on Self-Harm Treatment
Since self-harm is not a mental health condition of its own, tracking treatment statistics is challenging. What experts do know is thattreatmentmust focus on the factors that trigger self-harm, as well as the self-harm itself.
For example, if yourself-harm is connected to substance use, getting help from The Recovery Village could reduce self-harm as you find recovery from alcohol and other drugs.Call todayto speak to a representative about available treatment options for self-harm and substance use disorders.
Question of the day - What do you think is the most important skill to learn for resiliency?
Self Harm & Self Sabotage
What do you think is the most important skill to learn for resiliency?
Daily archives
Current Survey
Top 5 Contributors (Jan)

22448 pts

20209 pts

14197 pts

12060 pts

11932 pts